 LOGIN
LOGIN REGISTER
REGISTER.png)


Case Report
The Isotopic Coresponse Phenomenon
Ouiame El jouari*, Ghita Senhaji, Zakia Douhi, Sara Elloudi, Hanane Baybay, Fatima zahra Mernissi.
Department of Dermatology, University Hospital Hassan II, Fez, Morocco
*Corresponding Author: Ouiame El jouari, Department of Dermatology, University Hospital Hassan II, Fez, Morocco. E-mail : eljouariouiame88@gmail.com
Citation : jouari OE, Senhaji G, Douhi Z, Elloudi S, Baybay H et al. (2019) The isotopic coresponse phenomenon. J Dermatol Surg Res Ther, 2019 : 53-59.
Received Date : 29 November, 2018 ; Accepted Date : 30 January, 2019 ; Published Date : 08 March, 2019
Abstract
The isotopic coresponse phenomenon is an unusual condition in clinical practice, rarely reported in the literature. It is defined as the presentation of a dermatosis that develops in the same area of skin as another previously present but still active dermatosis. The etiology and pathogenesis are still unknown. Only 4 cases of the isotopic coresponse phenomenon are reported in the literature. We report a very unusual colocalization between vitiligo and lichen planus hypertrophic.
Keywords
Vitiligo; hypertrophic lichen; isotopic response phenomenon.
Introduction
The appearance of a skin condition on the same anatomical site of an earlier dermatosis has recently been called the isotopic coresponse phenomenon [1]. The pathogenesis of this phenomenon is still unknown. Few cases describe this entity; we have found 4 reports in the literature [2]. Colocalization between lichen and vitiligo is very unusual, especially the hypertrophic variety. We describe a particular case of a young man developing two different entities at the same site.
Case presentation
A 22-year-old male with 6 years’ history of goiter in euthyroid and vitiligo, put on dermo corticoids and UVB phototherapy then relay by Tacrolimus, with a favorable response and persistence of a single achromic macula in the right knee. The evolution was marked by the appearance 4 years later of a slightly itchy hypertrophic plaque on the achromic macula. The dermatological examination had revealed a 6 cm hypopigmented macula with irregular contours, repigmentation islands and leukotrichia, located on the anterolateral side of the knee. This macula was surmounted by a 5 cm hypertrophic erythematous squamous plaque of irregular contours with a peripheral hyperpigmented halo [Figure 1].
|
Figure 1: a 6 cm hypopigmented macula surmounted by hypertrophic erythematous squamous plaque with a peripheral hyperpigmented halo. |

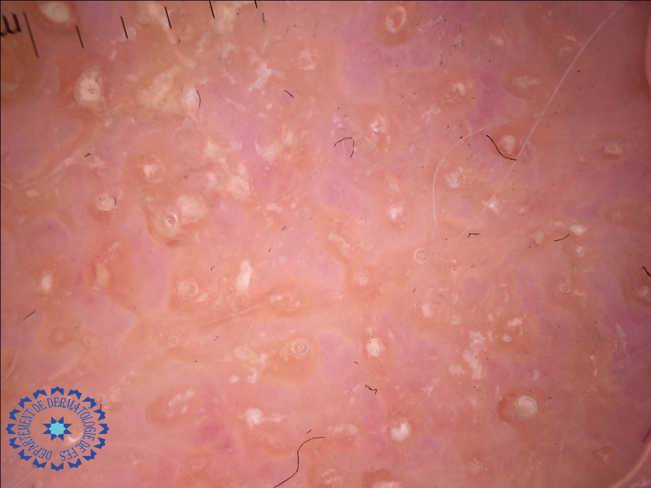
The examination of mucous membranes and phaneres was normal with no palpable lymphadenopathy. The dermoscopy showed an erythematous background, yellowish structure surrounded by irregular linear vessels [Figure 2].
|
Figure 2: erythematous background, yellowish structure surrounded by irregular linear vessels. |
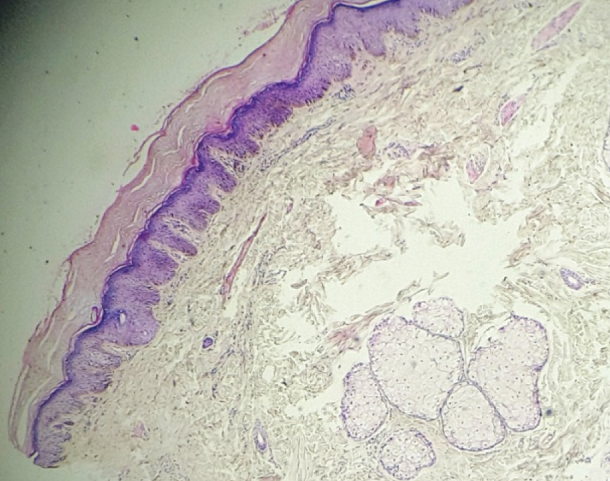
Histological examination had objectified epidermis with hyperkeratosis, mild increase in the granular layer, acanthosis areas, foci of degeneration in the basal layer, subepidermal cleft, mild lymph histiocytic infiltrate in the superficial dermis [Figure 3].
|
Figure 3: Histological findings showing hyperkeratosis with acanthosis areas, foci of degeneration in the basal layer, subepidermal cleft, mild lymph histiocytic infiltrate in the superficial dermis. |
The diagnosis of hypertrophic lichen was made. The patient had received CO2 laser sessions with simultaneous intralesional injection of 10 mg of triamcinolone actonide. The evolution was marked by the regression of the hypertrophic plaque and the improvement of the macule of vitiligo.
Discussion
The development of skin lesions at the same site as a distinct previous dermatosis, with no relationship between the 2 conditions, has been described as the Wolf isotopic response [3]. The isotopic response describes the eruption of a secondary, pathogenically distinct cutaneous disorder within the borders of a previous, already healed skin disease [4]. It may be considered as a particular variant of Kobner phenomenon, in which one cutaneous disorder induced a second one [4]. According to the new classification, this phenomenon is defined by the appearance of skin diseases at the same anatomic site as other previous dermatoses [3]. The isotopic coresponse phenomenon differs from the classic Wolf isotopic response in that the first disease is still active at the time of appearance of the second skin disease [5]. The etiology and pathogenesis are still unknown [6], several theories currently explain this rare and interesting phenomenon. The koebnerization theory and the actinic damage theory are among the most commonly cited in the literature. Although alteration of immunity limited to the site of the lesions can be incriminated [6]. The most common pathologies that can occur in the same site, are granulomatous and lichenoid reactions, infiltration of hematologic diseases, skin tumors and infections [2]. Only 4 cases of the isotopic co-response phenomenon are reported in the literature. The 4 cases described an association of vitiligo with lichen planus [5]. Lichen planus colocalized with vitiligo is poorly reported in the literature, moreover the hypertrophic variant. We present a rare case of this unusual colocalization between hypertrophic subtype of lichen planus and vitiligo. Vitiligo is an auto-immune pigmentary disease acquired secondary to destruction of melanocytes. Lichen planus hypertrophic is considered a rare subtype of lichen planus manifests by pruritic purple-grey colored keratotic plaques covered with fine adherent scales, appears frequently on the pretibial areas and ankles and appears often more resistant to standard topical treatment [7]. Several theories have been proposed to explain this phenomenon. Why the isotopic response phenomenon is not seen in all people ? Does the Kobner phenomenon has a role in this collocation? is there any contribution of genetic, environmental, alimentory factors and other unknowns? Persistent immunological changes, such as lymphocyte memory cells, are they implicated in the occurrence of the second dermatitis ? the implicated may be that vascular changes predisposes the skin to develop a second distinct disorder at the same site. we could not establish a relationship between the occurrence of these 2 diseases on the same site. Further studies are needed [2]. In our case, we have opted for a treatment that will act on both pathologies.
Conclusion
The isotopic coresponse phenomenon is an unusual condition, rarely reported in the literature. The interest of this presentation is to recognize this particular phenomenon. Our presentation is atypical by the hypertrophic type of lichen planus and other observation are needed to explain the colocalization of the two diseases.
References
- Kluger N (2018) Phenomena of Köbner, Renbök, Wolf and Co. ... is it time to simplify? Köbner, Renbök, Wolf phenomena and so on ... has the time come for simplification? Annals of dermatology and Venereology, 145: 347-353.
- Queiroz MTS, Almeida JRP, Sementilli A, Mattos e Dinato SL, Romiti N (2015) Wolf’s isotopic response, presenting as lichen planus. An Bras Dermatol, 90 (3 Suppl 1) : S91-93.
- Oscoz JS, Loidi PL, Tun ?ón AMT, Yanguas BJI (2016) Liquen nitidus sobre vitíligo: nueva variante del fenómeno de co-respuesta isotópica. Actas Dermosifil- iogr, 107: 860-861.
- Kroth J, Tischer J, Samtleben W, Weiss C, Ruzicka T et al. (2011) Isotopic response, Kobner phenomenon and Renbok phenomenon following herpes zoster. Journal of Dermatology, 38: 1058–1061.
- Kannangara AP, Yosipovitch G, Fleischer AB (2014) Proposed classification for Koebner, Wolf isotopic, Renbok, Koebner nonreaction, isotopic nonreaction and other related phenomenon. Dermatol on J, 20, pii: 13030/qt96s656b4.
- Jaka MA, López Pa A, López N ez M, Ormaechea PN, Vildosola ES et al. (2012) Wolf isotopic phenomenon: 9 cases seriesWolf's Isotopic Response: A Series of 9 Cases. Actas Dermosifiliogr, 103: 798-805.
- Alamri A, Alsenaid A, Ruzicka T, Wolf R (2016) Hypertrophic lichen planus – successful treatment with acitretin. Dermatol Ther, 29 : 173–176.